 Request Appointment
Request AppointmentSurgical Treatments
Leading Surgical Care for Aortic Disease
We offer leading surgical care for both elective and emergent aortic procedures. Our team is also involved in research to identify new treatment options that can enhance the quality of life for patients.
Because disease of the aorta can cause problems all along its length, it is important to take into account future problems that may arise. This is why it is important to have a team that thinks about the whole aorta.
Surgery on the aorta has come a long way in the past few years. In many cases, there are minimally invasive techniques that allow surgeons to repair the aorta through tiny incisions. This is called endovascular surgery.
In some cases, open surgery is necessary. The specific size and location of the incision, the use of the heart-lung machine and other techniques vary depending on the type of aortic surgery being performed.
Stent Grafts
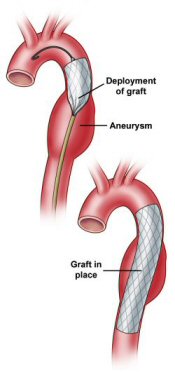 We also offers catheter-guided endoluminal stent grafts to repair aortic disease. These procedures are called Endovascular Aortic Repair (EVAR) and Thoracic Endovascular Repair (TEVAR). These stent grafts are inserted through a small incision in the groin and placed in the diseased aorta. Stent grafts allow faster and easier recovery.
We also offers catheter-guided endoluminal stent grafts to repair aortic disease. These procedures are called Endovascular Aortic Repair (EVAR) and Thoracic Endovascular Repair (TEVAR). These stent grafts are inserted through a small incision in the groin and placed in the diseased aorta. Stent grafts allow faster and easier recovery.
Complex endovascular repair is sometimes needed if the problem also involves the branches of the aorta. For this, special stents are used which have branches or holes (fenestrations) to maintain blood flow to the organs. This type of repair requires special expertise, which our teams provide.
Hypothermic Circulatory Arrest in Surgery
In aortic surgery it is sometimes necessary to perform procedures without clamping the aorta, while at the same time keeping the surgical field free of blood. An effective solution was found in hypothermic circulatory arrest (HCA), also called total circulatory arrest (TCA).
Hypothermic circulatory arrest uses very cold body temperatures to temporarily suspend blood flow. Cold temperatures slow cellular activity significantly, and blood circulation can be stopped for up to 40 minutes without harm. This allows surgery to be performed safely on the aorta when clamping to contain blood flow is either impossible or not the preferred approach.
The open anastomosis (surgical connection) technique for ascending aortic dissection surgery is now the favored approach. Using HCA the ascending aorta is not clamped while the aneurysm is surgically removed (resected) and the graft is sewn to the aortic arch.

Aortic Valve, Root, Ascending Aorta and Arch
Aortic disease often involves more than one location. It may simultaneously affect the aortic valve, root, ascending aorta and/or arch. The arteries that branch from these aortic segments require special consideration during surgery. This includes the coronary arteries, which supply blood to the heart, as well as the arteries branching form the arch, which supply blood to the head and upper body. A combination of procedures may be used during surgery.
The aortic root contains the aortic valve and gives rise to the coronary arteries that supply blood to the heart muscle. There are currently two main valve sparing root operations: the aortic valve reimplantation (David I) and the aortic valve remodeling procedure (David II, Yacoub). There are also several variations of both procedures that we use at VCU Health, as appropriate.
Options
Aortic surgery may be elective (scheduled) or emergent. Elective surgery is chosen to prevent devastating complications such as aortic rupture and tearing. Emergency surgery is necessary to repair life-threatening complications of aortic disease. These procedures include repair of aortic dissection, replacement of the aortic valve and repair of a ruptured aneurysm.
Timing of Elective Surgery
Managing aortic disease requires deciding whether the risk of rupture or dissection is greater than the risk of surgery. Improved surgical outcomes allow surgeries to be performed earlier today than in the past, operating before life-threatening rupture or dissection occurs. In determining the timing of surgery, the overall condition of the individual and their aortic tissue is evaluated. Factors considered include:
- Size of aneurysm
- Shape of aneurysm
- Rate of expansion
- Family history of aortic rupture or dissection
- Type of aortic disease
- Patient age and general health
- Symptoms - pressure or pain in the chest, abdomen, or back