Celebrating 50 Years of Heart Transplantation
On the afternoon of May 25, 1968, something mysterious was taking place on the 11th floor of MCV’s West Hospital.
An elevator operator was prohibited from taking visitors to the floor, which was secured by guards. From a landing on the stairwell outside the 11th floor, reporters caught glimpses of doctors and nurses in blue surgical scrubs moving rapidly down the corridors when the guards would briefly open the stairwell doors to let in interns and other hospital personnel. Later, they would learn that pioneering surgeon Dr. Richard Lower, had performed the first cardiac transplant in Virginia—just the 16th in the world.
Fifty years later, Lower’s legacy continues in the innovative work at Pauley, where 581 cardiac transplants have since taken place. While today the procedure is more commonplace—no reporters hunkering down in the stairwells—the event of human cardiac transplantation remains no less extraordinary.
Dr. Vigneshwar Kasirajan, chair of the Department of Surgery, maintains his office on the 16th floor of the storied West Hospital. A cardiothoracic surgeon, he holds great respect for the physicians who developed MCV into one of the first and foremost centers for organ transplantation—Lower, as well as Drs. David Hume, H.M. Lee, and others.
“They were giants in the field,” he said, sitting at a conference table in an alcove off his office. At the same time, he is excited about recent developments. “I want to talk about what’s been going on at VCU Health over the past few years and what’s ahead in the future for heart transplantation.”
We are experiencing a time of significant growth. In 2016, the hospital’s surgical teams performed 30 heart transplants and were anticipated to complete between 25 and 30 of the operations in 2017. The numbers include heart-kidney and heart-liver transplants.
“If you look at the trajectory, transplants are up 50% in just three to four years. Threefold from eight years ago. It’s a growing program with excellent outcomes.” — Dr. Keyur Shah
According to Kasirajan, “about 60-70% of our patients are still alive and fully functional after 10 years.”
At the same time, the transplant program is limited in its growth by the inadequate supply of donor hearts. On any given day, about 4,000 people in the U.S. are on the wait list for a human heart, but only 2,300 donor hearts are available each year. The wait time can range from six months to one year. Despite the greater public awareness of the need for organ donors, the shortage has remained constant for some time. But Kasirajan, Shah and others are not satisfied with the status quo—instead they keep pushing for new solutions to improve and extend the lives of patients in need of cardiac transplantation.
“The biggest thing that has happened with transplantation at Pauley over the last few years is the development of a comprehensive advanced heart failure and mechanical assist device program under the leadership of Drs. Keyur Shah, Richard Cooke and Daniel Tang.” — Dr. Vigneshwar Kasirajan.
Mechanical assist devices such as heart pumps and total artificial hearts are “bridge-to-transplants” that can buy time for patients with advanced heart failure until a donor heart becomes available.
The 1990s saw the boom of the left ventricular assist device. In 1994, Heart Mate I became the first such device approved by the FDA; VCU Medical Center implanted one that same year.
“Older LVADs were large, noisy and were only available to larger-sized people with large thoracic cavities,” said Shah. Today, LVADs can fit in the palm of the hand and can be implanted in those of a slighter stature. “They’re smaller, quieter and they’ve become more durable and longer lasting.”
Another game changer was the total artificial heart. In 2006, a surgical team led by Kasirajan implanted the first total artificial heart on the East Coast at VCU Medical Center. Today, the program is the third largest in the country.
About 50 LVADs and total artificial hearts are implanted in patients at VCU Medical Center each year. “The introduction of contemporary LVADs and the total artificial heart has been nothing short of revolutionary,” said Shah. “Prior to their development, patients would often die while waiting for the heart transplant list. Now, these patients who are critically ill can live for a long period of time, with a good quality of life, on these mechanical devices.”
Six clinical researchers take part in the busy heart failure program that prides itself on remaining at the cutting edge of device and pharmaceutical research.
“We have participated in clinical trials to implant devices through smaller incisions and are looking forward to participating in a study, hopefully this year, that will evaluate the smallest LVAD we’ve ever implanted in a person,” said Shah. “It’s been studied in Europe, but this would be the first U.S. trial.”
Another study soon to come is that of the Carmat heart, which was designed by noted French cardiologist and valve designer Dr. Alain Carpentier, in conjunction with EADS, the company behind aerospace leader Aerobus. Dubbed the world’s first self-regulating total artificial heart, the device uses embedded sensors and microprocessors to attune the rate of blood flow to patient needs—beating faster during exercise, for instance. It’s also designed to be more biocompatible, with bovine pericardium tissue on all surface areas that contact blood. This pump is electrically powered and has a quiet operation.
According to cardiothoracic surgeon Dr. Daniel Tang, “this would be the first U.S. trial for the device. They’ve done seven patients so far but none in the U.S. Our successful trials with SynCardia [another TAH manufacturer] is why Carmat reached out to us.”
Is it possible to stop or even reverse heart failure before it progresses? That’s a question that will be explored via a new trial that will soon begin in the cardiac catheterization lab. Dr. Zachary Gertz, director of the structural heart disease program, is investigating a therapy that may repair tissue damaged by heart attacks.
“We are about to be involved in the first real pivotal trial of interventional stem cell therapy,” said Gertz. Now in its third phase, the trial involves the injection of stem cells, a class of undifferentiated cells that can morph into other cell types and renew indefinitely.
“When you have a heart attack, a piece of heart muscle dies and it scars. There’s also this rim around it called the peri-infarction zone, which is also not getting good blood supply or working that well,” he explained. “The idea is that by injecting stem cells directly into this peri-infarct area, you might encourage that heart muscle to work better and improve the patient’s outcomes.”
Known as CardiAmp Therapy, the process begins by taking bone marrow out of a patient’s hip and placing it in a spinning device called a centrifuge. “This will give us back just the best cells, the ones we want to use,” he said. Those healthy cells will be transported to the heart by way of a catheter placed in the upper thigh. “There’s a second catheter that screws into 10 spots in that region encircling the area where the heart attack occurred. You can then inject the cells into each of those spots.”
The trial covers some potentially groundbreaking territory. “We’re going to encourage the reinvigoration of nearly dead heart muscle. No one’s been able to ever really do that before,” he said. “If it works, it will be pretty amazing.”
“Dr. Lower’s research and clinical efforts, before the first transplant, during the early days, and for decades afterward, shaped the field of heart transplantation. It affected things from surgical techniques to early immunosuppression, and he defined how to detect rejection and address complications after transplant. Dr. Szabolcs Szentpetery and he were involved in the first long-distance procurement of the heart—and the list goes on and on,” said Dr. Shah.
Sadly, since Lower’s time, little progress has been made in heart preservation, said Kasirajan. A heart can still only be stored for three to four hours. “There are 30 hearts that are discarded every year in Puerto Rico because they’re never used for transplantation. I can’t transfer a heart from Hawaii to the U.S., even if it’s the best match for a patient,” he said.
VCU Health’s new Christine B. and David E. Cottrell Surgical Innovation Laboratory will be created with the intent of not only improving heart preservation but also expanding the available donor pool. A $1 million donation by the Cottrells provided the lead gift as the Department of Surgery aspires to raise $4 million for the modernization and expansion of the ninth floor of Sanger Hall, to include sophisticated labs and operating rooms for training, as well as space ideal for testing and implementation of new devices developed by private industry. An additional $4 million is being raised for an endowment to fund such research in perpetuity.
“The Cottrells’ gift is allowing us to continue to develop our space as a center for excellence for innovation in surgery and help our physicians really bring from the research arena into the clinical practice exciting new innovations in preservation and heart transplantations,” said Kasirajan.
The new lab will support the work of researchers like cardiothoracic surgeon Dr. Mohammed Quader, who is focusing on Donation after Circulatory Death—or “DCD”—hearts. “These are the hearts donated by individuals whose life support has been withdrawn due to futile outcome; they sustain cardiac arrest during this process,” said Quader. Currently, these hearts are not used for transplantation, “other than in maybe two or three centers in the world, that too on a very small scale.”
Brain death donors, who are the current standard heart donors for transplantation, continue to have blood flow to the heart even after pronouncement of brain death. They are the current standard heart donors for transplantation. When blood flow ceases to the heart and cardiac arrest ensues, as it does in the DCD process, the heart sustains cellular damage.
Researchers at VCU Health hope to halt that process. Quader is the principal investigator of three different research grants and leading teams focused on mitigating the ill effects of DCD heart injury. In collaboration with Dr. Stephano Toldo, he has successfully developed an animal DCD heart model and gathered fundamental data to further the study of DCD outside of the body. Through a Pauley Pilot Grant, he is comparing three different preservation solutions to determine which one will best protect the DCD heart. Finally, with Dr. Edward Lesnefsky, he received a four-year Merit Review Grant through the Hunter Holmes McGuire Veteran Affairs Medical Center to study a drug that temporarily paralyzes the mitochondria of DCD cells in an animal model to prevent cellular damage.
His passion for finding alternative sources of heart donors is driven by the patients he sees every day, especially those who are awaiting donor hearts. “I take care of these patients. Not being able to use a DCD donor heart, which I feel has the potential to be used successfully, bothers me,” said Quader. “If I can make these hearts available for transplantation, the future will be better for our patients.”
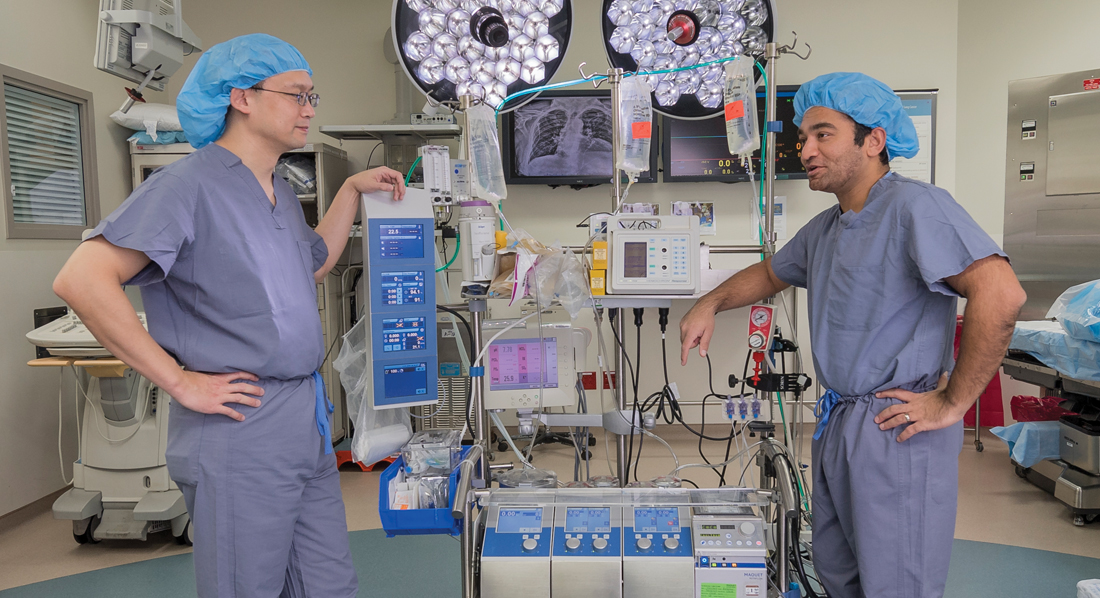
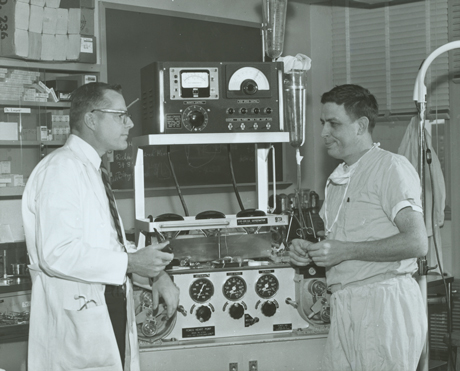
ABOVE: DR. DANIEL TANG (LEFT) AND DR. KEYUR SHAH, WITH A MODERN HEART-LUNG BYPASS MACHINE; ABOVE RIGHT: DR. RICHARD LOWER (LEFT) AND DR. RICHARD CLEVELAND, WITH ITS PREDECESSOR: THE PEMCO HEART PUMP.
Back to Spring-2018